This section presents historical data and projections of the numbers of (1) persons applying for SSI payments; (2) new recipients of SSI payments as a result of an application; (3) terminations from SSI payment status; and, (4) recipients of federally administered SSI payments. These historical data and projections are presented by category and age group.
1 All of the corresponding tables are located at the end of this section.
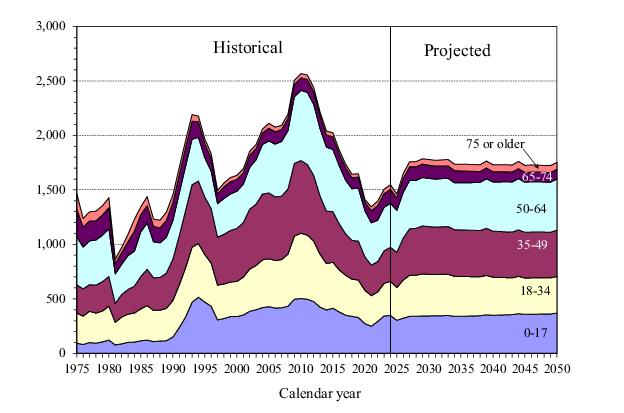
Figure IV.B1 presents historical and projected numbers of persons applying for SSI payments at SSA field offices, including applications taken by telephone and online, by calendar year.
3 The level of applications generally decreased from 2010 through 2019 as the economy recovered from the recession of 2007-2009. The number of applications decreased sharply in 2020 and remained low in 2021, due to a number of COVID-19 pandemic-related effects. Since 2021, the number of applications has increased moderately, which resulted from applications increasing substantially at ages 0 to 17 and increasing more moderately at ages 18 and older. In 2025, the number of applications is projected to decrease somewhat, reflecting recent experience in late 2024 and early 2025. In 2026 and 2027, the number of applications is projected to increase substantially, reaching levels more consistent with longer-term expected experience. The number of applications is projected to be 1.8 million in 2027, and then remain at roughly this level thereafter.
As part of SSA’s adjudication of these applications, the levels of income and resources available to the applicants are evaluated along with other eligibility factors including marital and citizenship status and living arrangements. In addition, generally about 90 percent of the SSI applications are for disability payments that require the State Disability Determination Services (DDS) to evaluate the alleged impairment(s). Applicants may appeal an unfavorable disability determination through several administrative levels of appeal. If applicants pursue all administrative levels of appeal without success, they may appeal to the Federal courts.
4 An applicant may decide at any point in this process to file a new application for benefits in lieu of continuing through the prescribed appeals process, generally provided that the individual does not currently have an appeal of an SSI application pending in this process.
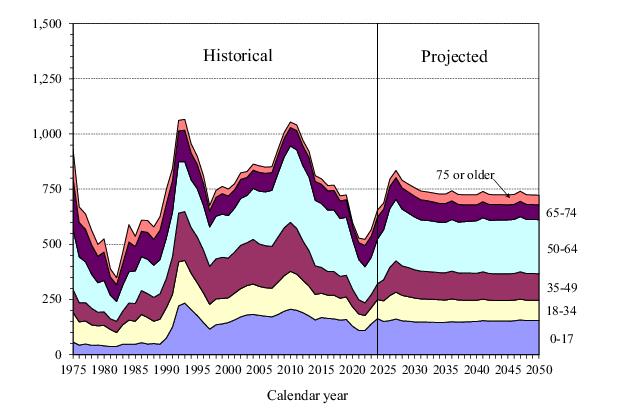
5Figure IV.B2 presents historical and projected numbers of persons who start receiving SSI payments as a result of this decision process.
6 The numbers of new recipients declined generally from 2010 to 2018, leveled off in 2019, decreased sharply in 2020 and 2021, and remained low in 2022, following the pattern of applications. The number of new recipients increased substantially in 2023 and 2024. The number of new recipients is projected to increase steadily to a temporary peak in 2027 as the time it takes the agency to adjudicate applications is assumed to decrease from recent high levels. From 2027 to 2031, the number of new recipients is projected to decrease gradually from 2027 to 2031 and then stay fairly level through the remainder of the projection period, despite the growing size of the U.S. population potentially eligible for SSI based on citizenship and residency requirements. This reflects the effects of the same factors assumed to affect the level of projected applications, as discussed previously. The projected numbers of new recipients throughout the projection period reflect the expected effects of the regulatory change to reduce from 15 years to 5 years the period of time that SSA will consider for past relevant work in the disability adjudication process.
7 We estimate this regulatory change will increase the number of new recipients from blind and disabled applicants throughout the projection period.
Some persons receiving SSI payments in a year will stop receiving payments during the year because of death or the loss of SSI eligibility. SSA uses three primary tools to assess continuing eligibility: (1) a non-medical redetermination, including limited issues; (2) a medical continuing disability review (CDR); and (3) medical redeterminations of SSI child recipients at age 18 using the adult initial disability criteria.
8 In a non-medical redetermination, the recipient’s non-medical factors of eligibility are reexamined, including income, resources, and living arrangements. In a medical CDR, the recipient’s medical condition is reevaluated to determine whether the recipient continues to meet the Act’s definition of disability. Medical redeterminations of disabled children attaining age 18 evaluate whether such recipients qualify for payments using the adult medical eligibility criteria. The net reduction in the number of SSI recipients in
current-payment status during a period is referred to as the number of SSI terminations for that period.
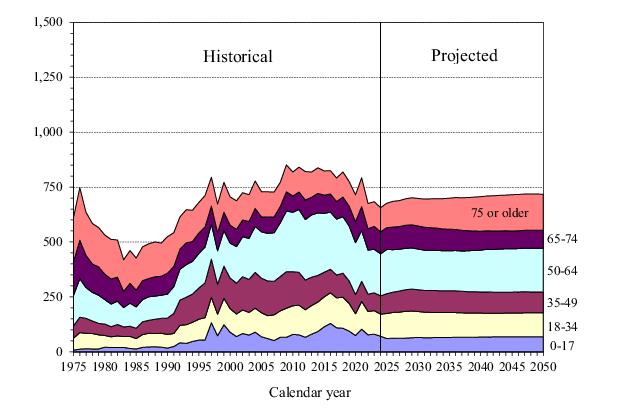
Figure IV.B3 presents historical and projected numbers of total terminations by calendar year.
9 The total number of terminations of federally administered recipients in 2024 decreased from 2023, by about 4 percent. Both the number of terminations due to death and the net number of terminations for all other reasons decreased by about 4 percent in 2024 compared to 2023. The net number of terminations for reasons other than death decreased largely because SSA performed fewer continuing disability reviews for SSI recipients in 2024 relative to recent years.
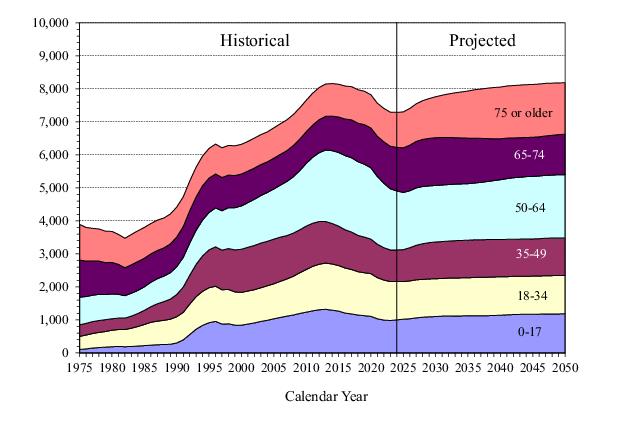
The number of SSI recipients receiving Federal payments increased rapidly in the early 1990s mainly due to the growth in the numbers of disabled adults and children. The growth in the numbers of children receiving SSI resulted in large part from the Supreme Court decision in the case of Sullivan v. Zebley, 110 S. Ct. 885 (1990), which greatly expanded the criteria used for determining disability for children. The growth in the numbers of disabled adults is a more complicated phenomenon. Extensive research conducted under contract to SSA and the Department of Health and Human Services suggested that this growth was the result of a combination of factors including: (1) demographic trends; (2) a downturn in the economy in the late 1980s and early 1990s; (3) long-term structural changes in the economy; and (4) changes in other support programs (in particular, the reduction or elimination of general assistance programs in certain States).
11 12 The 1996 welfare reform legislation, the economic downturn in the early 2000s, the economic recession that began in 2007, the subsequent economic recovery, and the COVID-19 pandemic beginning in 2020, have contributed to the more recent changes in program participation.
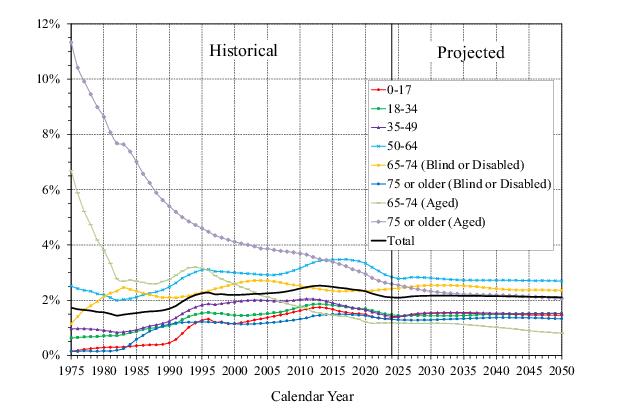
In order to place this projected growth in the context of overall population growth, figure IV.B5 presents Federal SSI prevalence rates by age group, defined as SSI recipients with Federal payments in current-payment status as percentages of the total Social Security area population for each age group.
13
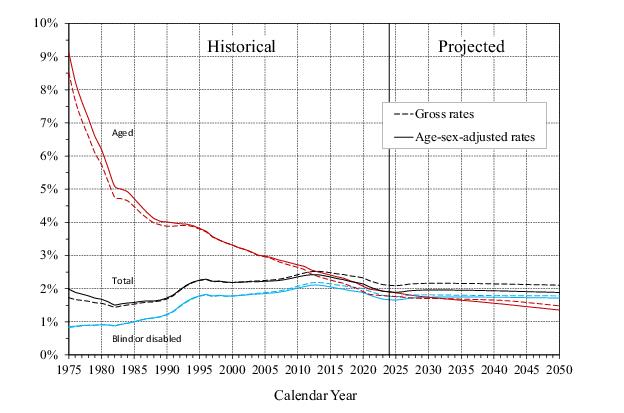
Figure IV.B6 presents prevalence rates for the two eligibility categories -
blind and disabled and
aged14 - as well as for the SSI program as a whole. It also shows these rates on an age-sex-adjusted basis, adjusted to the age-sex distribution of the Social Security area population for the year 2000. Adjusting these rates in this manner is useful when comparing rates over a long period of time because the age-sex-adjusted rates control for the effects that a changing age-sex distribution in the population can have on prevalence rates over time. That adjustment, however, does not account for the change over time of other factors that may affect the percentage of the Social Security area population that is SSI eligible.
Figure IV.B6 shows that the age-sex adjustment does not fundamentally change the overall pattern of the prevalence rates. The total SSI prevalence rate on an age-sex adjusted basis is higher before 2000 and lower after 2000 than the gross prevalence rate due to the changing age distribution of the population. The adjustment generally results in a more noticeable effect for the aged, especially in the early years of the SSI program, because the prevalence rate for ages 75 and older was much higher than for ages 65 to 74.
The prevalence rates for the eligibility categories of Federal SSI recipients follow significantly different growth patterns. The overall aged prevalence rate has declined steadily throughout the historical period, a trend that continues throughout the projection period. In contrast, except for decreases in the late 1990s due to the medical eligibility redeterminations and CDRs mandated by Public Law 104-193, the prevalence rate for blind or disabled children increased steadily through 2013, with the increase being relatively steep in the early 1990s. The prevalence rate for child recipients decreased slightly each year from 2014 through 2023, which is primarily attributable to the increased number of medical CDRs for these children, and the drop in applications and new recipients during most of this period. The total blind or disabled prevalence rate (as a percentage of the total Social Security area population at all ages) remained fairly level until the early 1980s, when it started increasing and then continued to increase through 1996. The blind or disabled prevalence rate declined slightly in the late 1990s due to the effects of welfare reform legislation but resumed an upward trend in 2000. That upward trend continued through 2013, but experienced slight decreases in 2014 through 2024. The projected overall prevalence rate for blind or disabled recipients decreases slightly through 2026, increases slightly through 2029, and then gradually declines throughout the remainder of the projection period due to assumptions that: (1) the population potentially eligible for SSI (i.e., the population meeting citizenship and residency requirements) will grow more slowly than the overall Social Security area population, (2) a smaller proportion of the population will become new recipients than during the 2007-2009 economic recession; (3) the age distribution of the population will change; and (4) SSA will receive sufficient administrative funding to process medical CDR and non-medical redetermination workloads, and those authorized resources will continue to be appropriated through the 25-year projection period.
15The total number of federally administered SSI recipients includes recipients only receiving a federally administered State supplement, as well as those receiving a Federal payment. Table IV.B8 presents historical and projected numbers of individuals who receive only a federally administered State supplement. Such recipients have countable income that exceeds the Federal benefit rate but which is lower than the combined amount of the Federal benefit rate and the State supplementary benefit level. These individuals must meet all other criteria required in order to be eligible for a Federal SSI payment. The vast majority of these individuals are concurrently beneficiaries of OASDI benefits. The historical and projected numbers do not include individuals eligible for only a state supplement that is not administered by SSA.
Table IV.B9 displays the combined numbers of persons receiving either a Federal SSI payment or a federally administered State supplement. This is the total number of SSI recipients with a benefit administered by SSA, which follows largely the same patterns of growth as the number of recipients receiving a Federal payment.